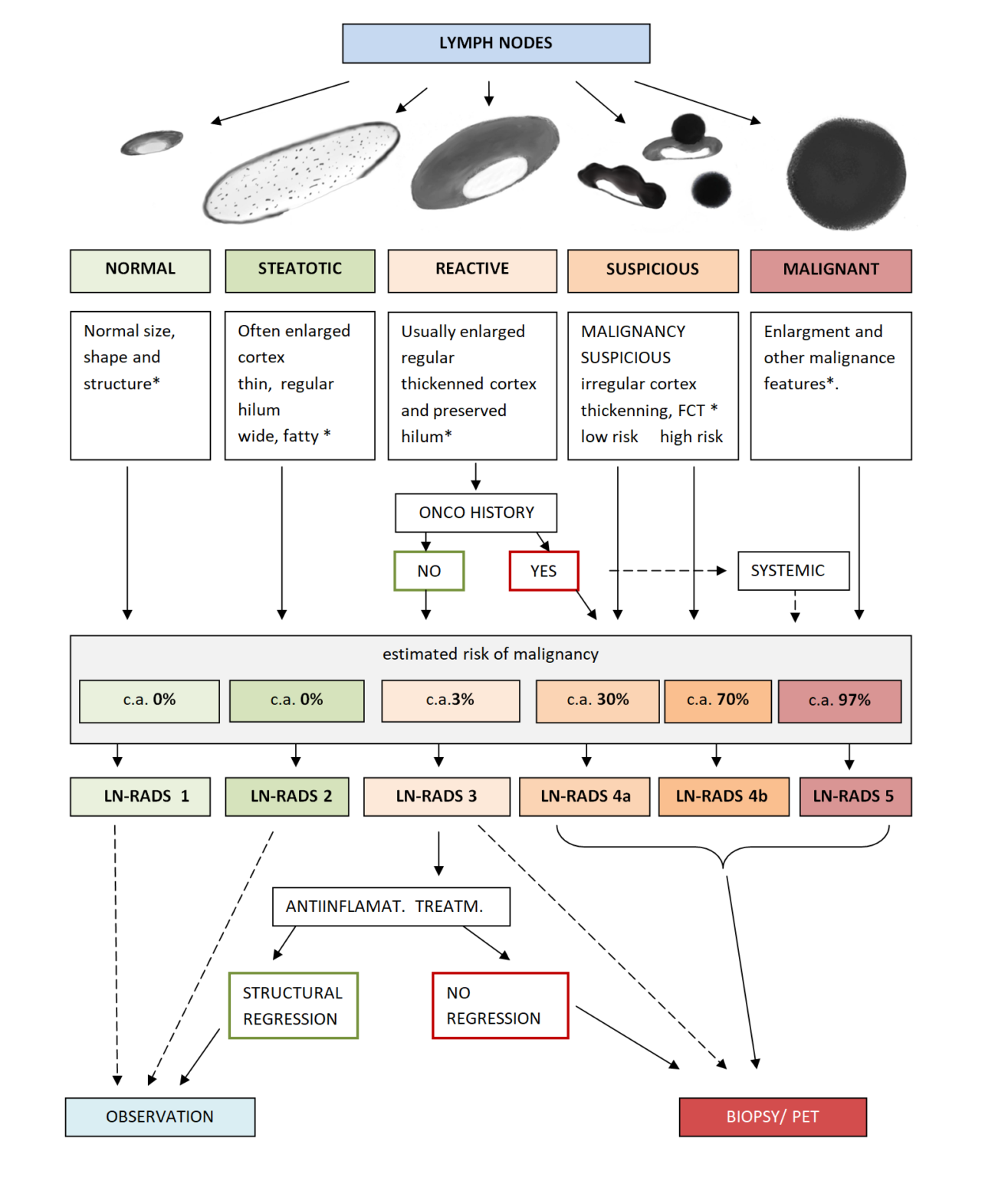
No enlargement (recommended max SAD up to 6-7mm), oval shape (L/S-ratio > 2), regular cortex, max. thickness ≤3mm, cortex echogenicity similar or higher to the background fatty tissue, smooth margins, no other changes in architecture (no calcifications, no fluid collections, no necrosis, no FCT), no pathological peripheral or chaotic vascularization.
LN-RADS 2 steatotic LN
LNs enlarged in one or both axes, cortex regular, max thickness ≤3mm, hyperechoic hilum (steatotic) with no size limits, no other changes in architecture (no calcifications, no fluid collections, no necrosis, no FCT, no pathological peripheral or chaotic vascularization).
LN-RADS 3 reactive LN
Probably due to the inflammatory process or vaccination. Dominant feature: regular, thickened cortex >3mm, enlargement in one or two axes, preserved oval shape (L/S-ratio > 2), preserved medulla, no other changes in architecture (no calcifications, no fluid collections, no necrosis, no FCT), cortical echogenicity similar to or moderately lower than the background fatty tissue, well-defined margins, no pathological peripheral or chaotic vascularization, no oncological or hematological history, no laboratory oncological abnormalities.
LN-RADS 4 suspicious LN
4a low, 4b high probability of malignancy. This group is dedicated to LNs that morphologically do not match groups 1, 2, 3, 5 or have additional radiological or clinical factors increasing the probability of malignancy in LNs categorized as LN-RADS 3, i.e. high or increasing laboratory markers (i.e. PSA for inguinal LNs), active neoplasm in the region (i.e. breast cancer for axillary LNs), other metastatic or systemic LNs in the region, clinical symptoms suggesting oncological or systemic hematological disease. The primary principle for categorizing LNs as group 4 is that “better check than miss”.
LN-RADS 4a
Low suspicion of malignancy – the size may be normal in SAD and LAD, cortex with thickening ≤4mm, moderate irregularity, especially local. As a general assumption, all LN 4a should be verified by biopsy or PET, and if it is not possible, they should be treated as suspicious and malignant.
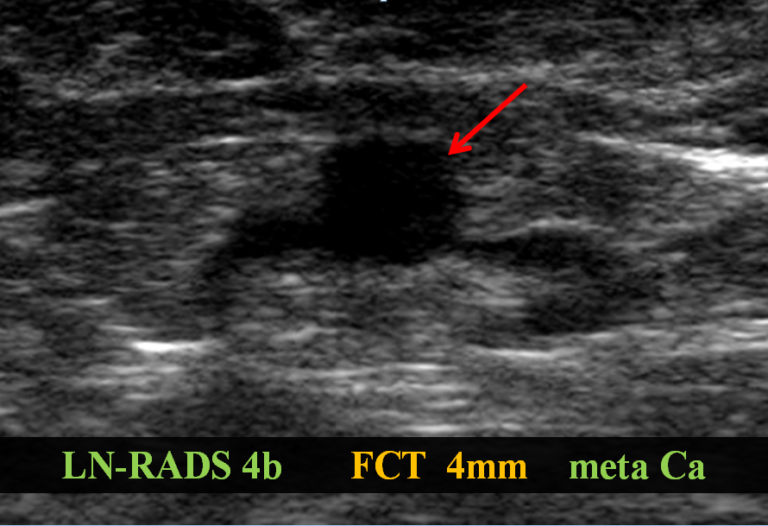
LN-RADS 4b
High suspicion of malignancy – the size may be normal in SAD and LAD, cortex thickening >4mm and irregularity, especially FCT, or no hilum, shape more round than oval (L/S-ratio≤2), hypoechogenicity to the background fatty tissue, especially “black hole sign”, microcalcifications, fluid collections, necrosis, abnormal peripheral or chaotic vascularization; ill-defined, blurred margin.
LN-RADS 5 malignant LN
Enlargement in SAD and one or more features of malignancy: lack of hilum, hypoechogenicity to the background fatty tissue or “black hole sign”, evident cortex irregularity /FCT”, shape more round than oval (L/S-ratio≤2), microcalcifications, fluid collections, necrosis, abnormal peripheral or chaotic vascularization; ill-defined, blurred borders or signs of extracapsular infiltration.
If evident radiological and clinical features of malignancy are present, enlargement is not necessary for LN-RADS 5 classification.